The Moral Imperative Towards Cost-Effectiveness
This essay by Toby Ord was published in March 2013 at the Center For Global Development and again in October 2019 in Effective Altruism: Philosophical Issues.
This essay explores the moral relevance of cost-effectiveness, a major tool for capturing the relationship between resources and outcomes, by illustrating what is lost in moral terms for global health when cost-effectiveness is ignored.
Full essay
Cost-effectiveness is one of the most morally important issues in global health. This claim will be surprising to many, since conversations about the ethics of global health usually focus on more traditional moral issues such as justice, equality, and freedom. While these issues are also important, they are often overshadowed by cost-effectiveness. In this note, I shall explain how this happens and what it means for global health.
The cost-effectiveness landscape in global health
The importance of cost-effectiveness is due to the fact that it varies so much between different interventions. Let us start with a simplified example to show how this becomes a moral consideration. Suppose we have a $40,000 budget which we can spend as we wish to fight blindness. One thing we could do is to provide guide dogs to blind people in the United States to help them overcome their disability. This costs about $40,000 due to the training required for the dog and its recipient.[1]
Another option is to pay for surgeries to reverse the effects of trachoma in Africa. This costs less than $20 per patient cured.[2] There are many other options, but for simplicity, let us just consider these two.
We could thus use our entire budget to provide a single guide dog, helping one person overcome the challenges of blindness, or we could use it to cure more than 2,000 people of blindness. If we think that people have equal moral value, then the second option is more than 2,000 times better than the first. Put another way, the first option squanders about 99.95% of the value that we could have produced. This example illustrates the basic point, but it is also unrealistic in a couple of ways. Firstly, it is rare for treatments in the United States to be traded off against treatments elsewhere. A health budget is normally more restricted than this, with a constraint that it is only spent on people in a particular rich country, or only spent on people in a designated category of poor countries. Secondly, we often have a spectrum of options. Thirdly, and most importantly, the class of interventions under consideration is often broad enough that it is difficult to make direct ‘apples to apples’ comparisons between the effects of two interventions.
Health economists and moral philosophers have an answer to the third of these issues. They use measures of health benefits that are powerful enough to be able to compare the values any two health benefits. The standard measure in global health is the Disability Adjusted Life Year (DALY). This measures the disvalue of health conditions in terms of the number of years of life lost due to the condition plus the number of years lived with disability multiplied by a number representing the severity of the disability. For example, a condition that caused one to die 5 years prematurely and to live the last 10 years with deafness would be valued as 5 + (10 x 33.3%) = 8.33 DALYs.
There are a number of complications and choices regarding the calculation of DALYs, which given rise to a number of subtly different versions of DALYs and the closely related units called QALYs. Chief among these is the question of the size of the weightings representing how bad it is on average to suffer from a particular disability. There are also considerations about discount rates and age weightings. Different reasonable choices on these parameters could change the number of DALYs due to a condition by a few percent or by as much as a factor of two. DALYs should thus be considered only as a rough measure of the disvalue of different conditions. It might seem that there would be little use for so rough a measure. This would be true if the difference in cost-effectiveness between interventions were also about a factor of two, but since it is often a factor of a hundred or more, a rough measure is perfectly adequate for making the key comparisons.
Let us now address all of the three concerns, by looking at a real world example of funding the prevention or treatment of HIV and AIDS. Let us consider four intervention types: surgical treatment for Kaposi’s sarcoma (an AIDS defining illness), antiretroviral therapy to fight the virus in infected people, prevention of transmission of HIV from mother to child during pregnancy, condom distribution to prevent transmission more generally, and education for high risk groups such as sex workers. It is initially very unclear which of these interventions would be best to fund, and one might assume that they are roughly equal in importance. However, the most comprehensive compendium on cost-effectiveness in global health, Disease Control Priorities in Developing Countries 2nd edition (hereafter DCP2), lists their estimated cost-effectiveness as follows:[3]
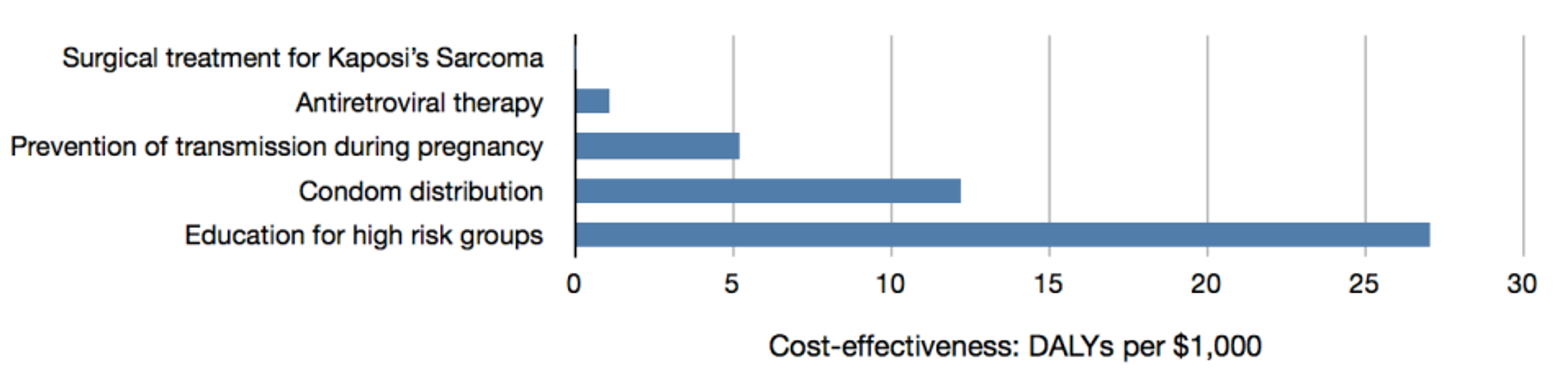
Note the wide discrepancies between the effectiveness of each intervention type. Treatment for Kaposi’s sarcoma cannot be seen on the chart at this scale, but that says more about the other interventions being good than about this treatment being bad: treating Kaposi’s sarcoma is considered cost-effective in a rich country setting. Antiretroviral therapy is estimated to be 50 times as effective as treatment of Kaposi’s sarcoma; prevention of transmission during pregnancy is 5 times as effective as this; condom distribution is about twice as effective as that; and education for high risk groups is about twice as effective again. In total, the best of these interventions is estimated to be 1,400 times as cost-effectiveness as the least good, or more than 1,400 times better than it would need to be in order to be funded in rich countries.
This discrepancy becomes even larger if we make comparisons between interventions targeted at different types of illness. DCP2 includes cost-effectiveness estimates for 108 health interventions, which are presented in the chart below, arranged from least effective to most effective.[4]
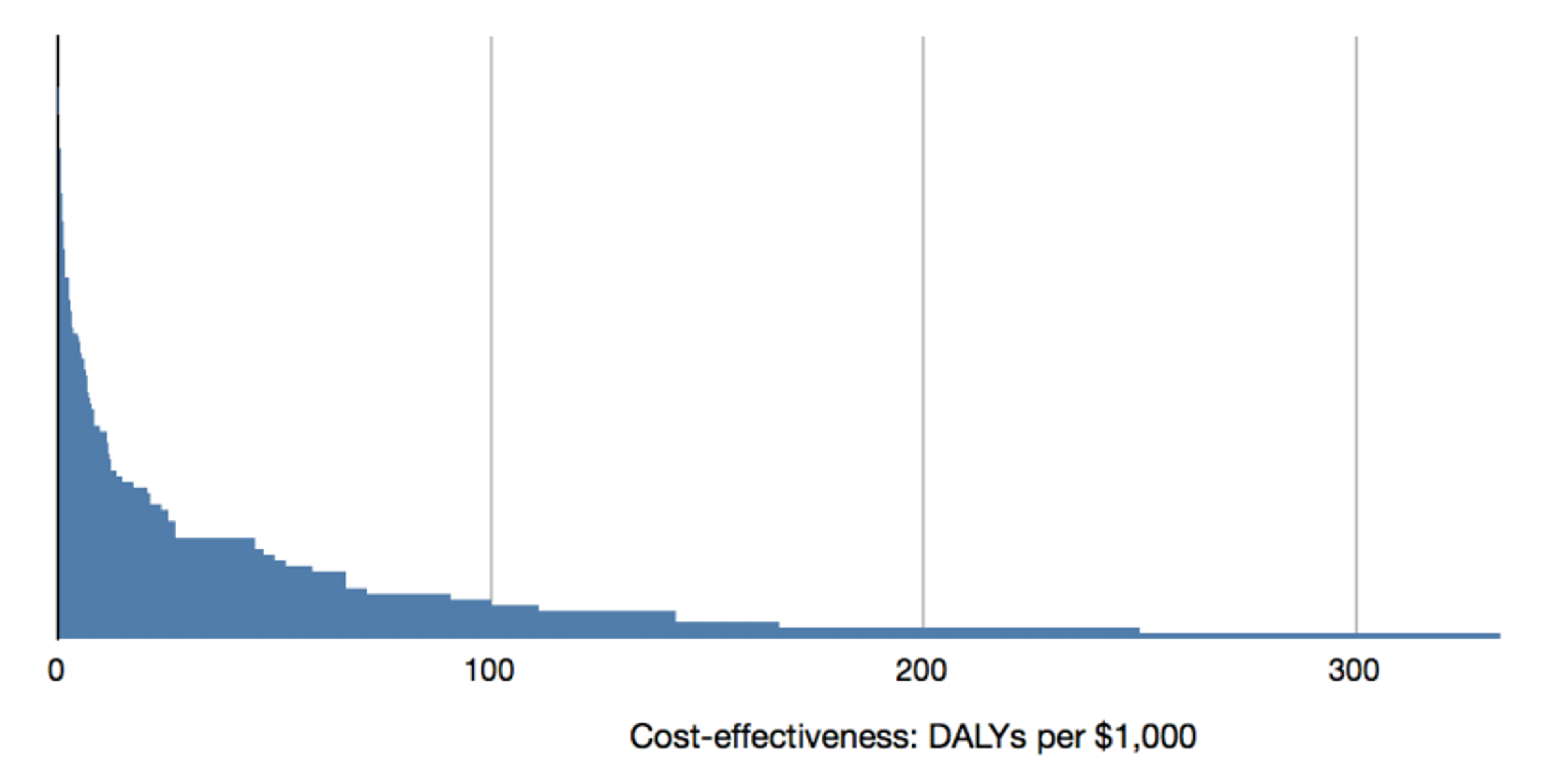
This larger sample of interventions is even more disparate in terms of costeffectiveness. The least effective intervention analysed is still the treatment for Kaposi’s sarcoma, but there are also interventions up to ten times more cost-effective than education for high risk groups. In total, the interventions are spread over more than four orders of magnitude, ranging from 0.02 to 300 DALYs per $1,000, with a median of 5. Thus, moving money from the least effective intervention to the most effective would produce about 15,000 times the benefit, and even moving it from the median intervention to the most effective would produce about 60 times the benefit. It can also be seen that due to the skewed distribution, the most effective interventions produce a disproportionate amount of the benefits. According to the DCP2 data, if we funded all of these interventions equally, 80% of the benefits would be produced by the top 20% of the interventions.
It must be noted that these are merely estimates of cost-effectiveness and there may be less variance between the real, underlying cost-effectiveness values. However, even if the most effective interventions are a tenth as effective as these figures suggest and the least effective are ten times better than they appear, there would still be a factor of 150 between them.
Moreover, there have been health interventions that are even more effective than any of those studied in the DCP2. For example, consider the progress that has been made on saving lives lost to immunization preventable illness, diarrhea, malaria, and smallpox, summarized in the following chart:[5]
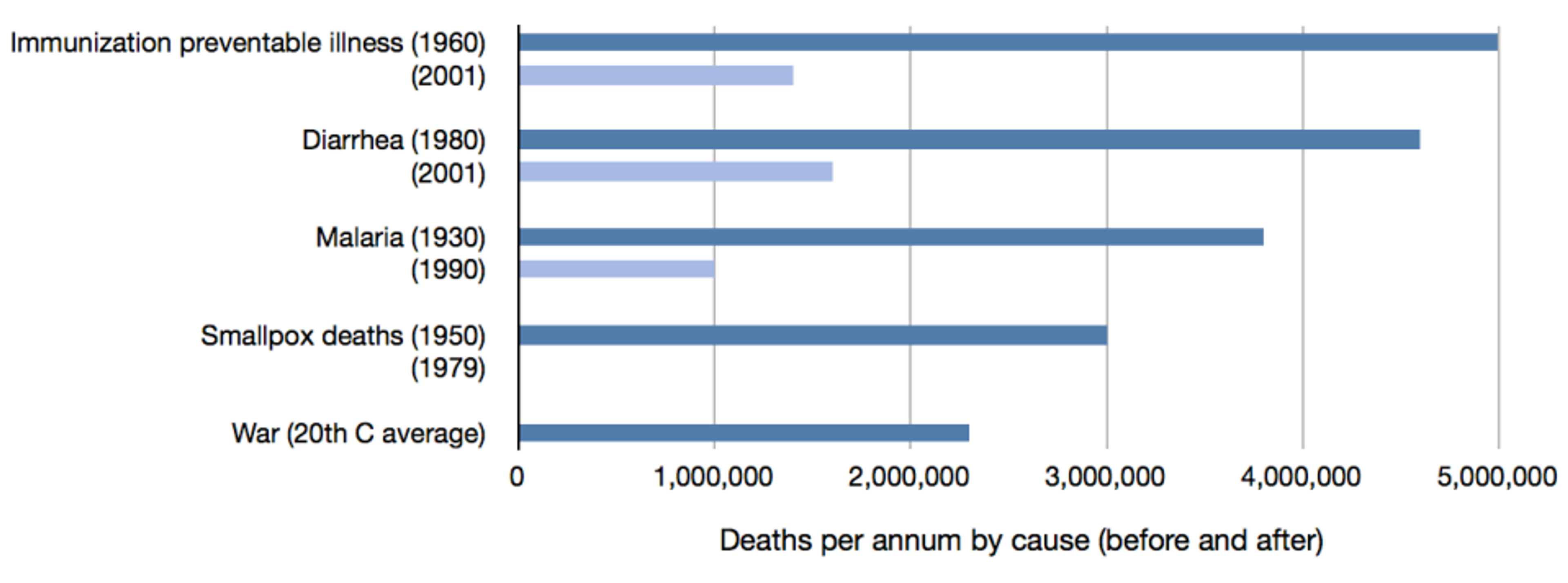
In all cases, our interventions have led to at least 2.5 million fewer deaths per year. To aid the reader in comprehending the scale of these achievements, I have added a final bar showing the average number of deaths per year due to war and genocide together over the 20 th Century (2.3 million). Thus, in each of the four of these disease areas, our health interventions save more lives than would be saved by a lasting world peace.
Moreover, these gains have been achieved very cheaply. For instance in the case of smallpox, the total cost of eradication was about $400 million.[6] Since more than 100 million lives have been saved so far, this has come to less than $4 per life saved — significantly superior to all interventions in the DCP2. Moreover, the eradication also saved significant amounts of money. Approximately $70 million was being spent across developing countries per year in routine vaccination and treatment for smallpox, and more than $1,000 million was lost per year in reduced productivity.[7] Even just in the United States, smallpox vaccination and vigilance cost $150 million per year before eradication.[8] The eradication programme thus saved more lives per year than are lost due to war, while saving money for both donors and recipients, paying back its entire costs every few months. It serves as an excellent proof of just how cost-effective global health can be.
The moral case
In these examples, we have seen how incredibly variable cost-effectiveness can be within global health. The least effective intervention in the HIV/AIDS case produces less than 0.1% of the value of the most effective, and if we are willing to look at different kinds of disease, this fraction drops to less than 0.01%. Ignoring costeffectiveness thus does not mean losing 10% or 20% of the potential value that a health budget could have achieved, but can easily mean losing 99% or more. Even choosing the median intervention can involve losing 85% of the potential value. In practical terms, this can mean hundreds, thousands, or millions of additional deaths due to failure to prioritize. In non-life-saving contexts it means thousands or millions of people with untreated disabling conditions.
Even when other ethical issues in global health are very important in absolute terms, they are typically much smaller than this. For instance, it may be worse on equity grounds to treat a million people in a relatively affluent city than to treat the same number of people spread between the city and the relatively much poorer rural areas. However, it is not vastly worse — not so bad that 99% of the value is lost. Learning how to correctly factor these other ethical issues into our decision making is an important and challenging problem, but we are currently failing at a much more basic, more obvious, and more important problem: choosing to help more people instead of fewer people, to produce a larger health benefit instead of a smaller one.
Challenges addressed
Some people don’t see cost-effectiveness as an ethical issue at all, since it is so cut and dried that it seems like a mere implementation issue. This is misguided. People who decide how to spend health budgets hold the lives or livelihoods of many other people in their hands. They are literally making life-or-death decisions. Most decisions of this sort take dramatically insufficient account of cost-effectiveness. As a result, thousands or millions of people die who otherwise would have lived. The few are saved at the expense of the many. It is typically done out of ignorance about the significance of the cost-effectiveness landscape rather than out of prejudice, but the effects are equally serious.
Some object that consequences are not the only thing that matters. For example, some people think that acting virtuously or avoiding violating rights matters too. However, all plausible ethical theories hold that consequences are an important input into moral decision-making, particularly when considering life or death situations, or those affecting thousands of people. Indeed these are precisely the types of cases in which people think that it may even become permissible to violate rights. However, in the cases under consideration, there is not even a conflict between producing a much greater good and acting virtuously or avoiding violating people’s rights. The consequences are thus of great moral importance, with no serious moral factors counting in the opposite direction. Proponents of all ethical theories should therefore agree about the moral importance of funding the most costeffective interventions.
People might also be concerned about the particular choices involved in estimating the benefits of different health interventions. For example, they may disagree about particular disability weights, or about the method for eliciting these weights, or about discounting health benefits, or weighting benefits depending on the age of the recipients, or whether other issues such as equality need to be factored in. However, none of this is in serious disagreement with the thrust of this note. Indeed I personally have many of the same concerns, but as mentioned earlier the practical choices we face often involve factors of ten or more between different interventions, so none of the modifications mentioned here will change the rankings very much. People who are concerned about the details of measuring cost-effectiveness should join with the cost-effectiveness community in improving these measures, rather than throwing out the baby with the bathwater, and leading to thousands of unnecessary deaths.
Another reason people might be initially suspicious of prioritisation based on costeffectiveness is through confusing it with cost-benefit analysis (CBA). The latter is an economic method for prioritisation which involves determining the benefits for each person in terms of how many dollars they would be willing to pay, adding these up, and then dividing by the total costs in order to produce a benefit-cost ratio in units of dollars per dollar. This method is ethically suspect as it considers benefits to wealthy people (or groups) to be worth more than comparable benefits to poorer people (or groups) since the wealthy are willing to pay more for a given benefit.
However, the cost-effectiveness I have discussed in this note is very different, and is a type of analysis known as cost-effectiveness analysis (CEA). This doesn’t convert benefits into dollars, but just provides a raw measure of the benefits in units such as DALYs per dollar, or lives saved per dollar. Thus the wealth of the recipients is not an input to the analysis and it doesn’t discriminate towards interventions that favour the wealthy.
People might remain suspicious of cost-effectiveness since it makes a connection between dollars and health (or even life itself). Making trade-offs between so-called sacred values such as life with non-sacred values such as money strikes many people as morally problematic. However, no such trade-off is made in cost-effectiveness analysis. Instead there is a budget constraint of some fixed number of dollars. The cost-effectiveness ratios help one to see how much benefit could be causally produced if this money were spent on different interventions — for example, saving one thousand lives or saving ten thousand lives. The only comparison that is made is between these benefits. Whether or not it is worth spending the budget to save ten thousand lives is not part of the analysis.
Conclusions
In many cases ignoring cost-effectiveness in global health means losing almost all the value that we could create. Thus there is a moral imperative to fund the most costeffective interventions. This doesn’t simply mean implementing the current interventions in the most cost-effective way possible, for the improvements that can be gained within a single intervention are quite small in comparison. It also doesn’t just mean doing retrospective measures of the cost-effectiveness of the interventions you fund as part of programme evaluation. Instead, it means actively searching the landscape of interventions that you are allowed to fund and diverting the bulk of the funds to the very best interventions. Ideally it also means expanding the domain of interventions under consideration to include all those which have been analysed.
The main effect of understanding the moral imperative towards cost-effectiveness is spending our budgets so as to produce greater health benefits, saving many more lives and preventing or treating more disabling conditions. However, it also shows a very interesting fact about global health funding. If we can save one thousand lives with one intervention and ten thousand with another at an equal price, then merely moving our funding from the first to the second saves nine thousand lives. Thus merely moving funding from one intervention to a more cost-effective one can produce almost as much benefit as adding an equal amount of additional funding. This is unintuitive since it isn’t the case when one option is merely 10% or 30% better than another. However, when one option is 10 times or 100 times better, as is often the case in global health, redirecting funding is so important that it is almost as good as adding new funding directly towards the superior intervention. In times of global austerity and shrinking budgets, it is good to know how much more can be done within existing ones.
References
- Joseph Cook, et al. 2006. ‘Loss of vision and hearing’ in Jamison et al. (eds.), 2006. Frank Fenner, et al. 1988. Smallpox and its eradication, (Geneva: World Health Organisation).
- Dean Jamison, et al. (eds.), 2006. Disease control priorities in developing countries, 2 nd edn., (Oxford and New York: Oxford University Press).
- Prabhat Jha et al., 2004. ‘Health and economic benefits of an accelerated program of research to combat global infectious diseases’, Canadian Medical Association Journal 171:1203–8.
- Milton Leitenberg, 2006. ‘Deaths in wars and conflicts in the 20 th Century (3 rd ed.)’, Occasional Paper #29, Cornel University Peace Studies Program (Ithaca: Cornel University).
Publication
- Article: The Moral Imperative Toward Cost-Effectiveness in Global Health
- Author: Toby Ord
- Publication: Effective Altruism: Philosophical Issues
- Editors: Hilary Greaves and Theron Pummer
- DOI: 10.1093/oso/9780198841364.003.0002
- Print publication date: 2019
- Print ISBN-13: 9780198841364
- Published to Oxford Scholarship Online: October 2019