Charity Update II: Schistosomiasis Control Initiative (SCI)
This is the second of our series of charity updates. You can read the first one, on Development Media International, here.
The Schistosomiasis Control Initiative (SCI) has been one of our top recommended charities for several years now. Our colleagues at Givewell have published an extensive update on SCI recently that was generally very positive and SCI continues to rank among Givewell’s top charities.
In this blog post, we give you an update on their efforts that complements Givewell’s report. You can find more general information about SCI on our website. In our opinion, SCI continues to be one of the most effective charities in the world.
Updates on Effectiveness
Recent scientific findings related to SCI’s effectiveness
We have recently reported on new research indicating that treating schistosomiasis might reduce - with great effectiveness [1] - both malaria [2] and HIV [3] infections (due to reduced immunodeficiency and reduced female genital schistosomiasis). Even though such disease interaction had long been speculated about [4, 5], evidence for a causal connection and a cost effectiveness analysis had been lacking. In the light of this new evidence, we have increased confidence in recommending SCI, even though more research is needed on the topic.
It has also been suggested that schistosomiasis might interact with Tuberculosis [6], Hepatitis [7], and Appendicitis [8], all of which make up a substantial amount of the global burden of disease, and we are currently doing more research to look into these links. We are also re-investigating in how far schistosomiasis parasites contribute to undernutrition and lack of micronutrients.
However, some recent studies hint at a potential decrease in SCI’s effectiveness. A recent report [9] shows that climate change will make temperatures more suitable for schistosomiasis transmission over the next 20 years, not only in terms of spread to other currently non-endemic countries, but also in terms of increasing the intensities of the disease in countries currently affected. The authors suggest that this increase in infection and reinfection intensity may reduce the impact of control and elimination programmes such as those undertaken by SCI. On the other hand, the resulting increase in need and thus scalability of SCI’s programs might increase their effectiveness.
Furthermore, researchers continue to be worried about the development of drug resistance to praziquantel, as it is the only drug currently recommended by the World Health Organization for the treatment and control of human schistosomiasis, which is also used by SCI [10]. Some signs of resistance of schistosomes against praziquantel have been observed in the laboratory, but in the field only isolated cases of decreased effectiveness of praziquantel have been observed so far [10, 11]. However, these are not issues that decrease SCI’s effectiveness in the near future, as resistance is localized and limited.
Updates on Room for Additional Funding
The recent Givewell report on SCI estimates that SCI has room for $3.8-8.3 million of additional funding over the next few years. However, as the number of people targeted to receive deworming rises (see Figure 1), SCI could probably scale up and strengthen its efforts in the countries where they currently operate and expand to new countries.
A recent report by the World Health Organisation estimates that the overall costs for all kinds of preventive chemotherapy (i.e. mass deworming, not chemotherapy used as cancer treatment) in the coming year are in the hundreds of millions (see Figure 2). The investment target for preventive chemotherapy against schistosomiasis (for delivery only- medicines are donated by the pharmaceutical companies) during 2015–2020 is estimated to be about US$ 59 million (US$ 51–67 million) per year (see Figure 3). This already takes into account that countries such as Brazil and India completely covered the cost of distributing the donated medicines using their own resources.
In poorer countries such as the DRC, Senegal and Niger [12], costs of distributions are shared among the local Ministries of Health and SCI, as well as other organisations such as the USAID, END Fund, CNTD, and APOC. But poor countries are not in a position to execute these programs by themselves and bigger aid givers such USAID are also do not completely fund such programs. Thus, SCI, with their unique expertise, might play a substantial part implementing such future deworming programs and thus require substantially more funds. This could change in case bigger agencies such as USAID recognize the cost effectiveness of interventions targeting NTDs and star investing more in this area.
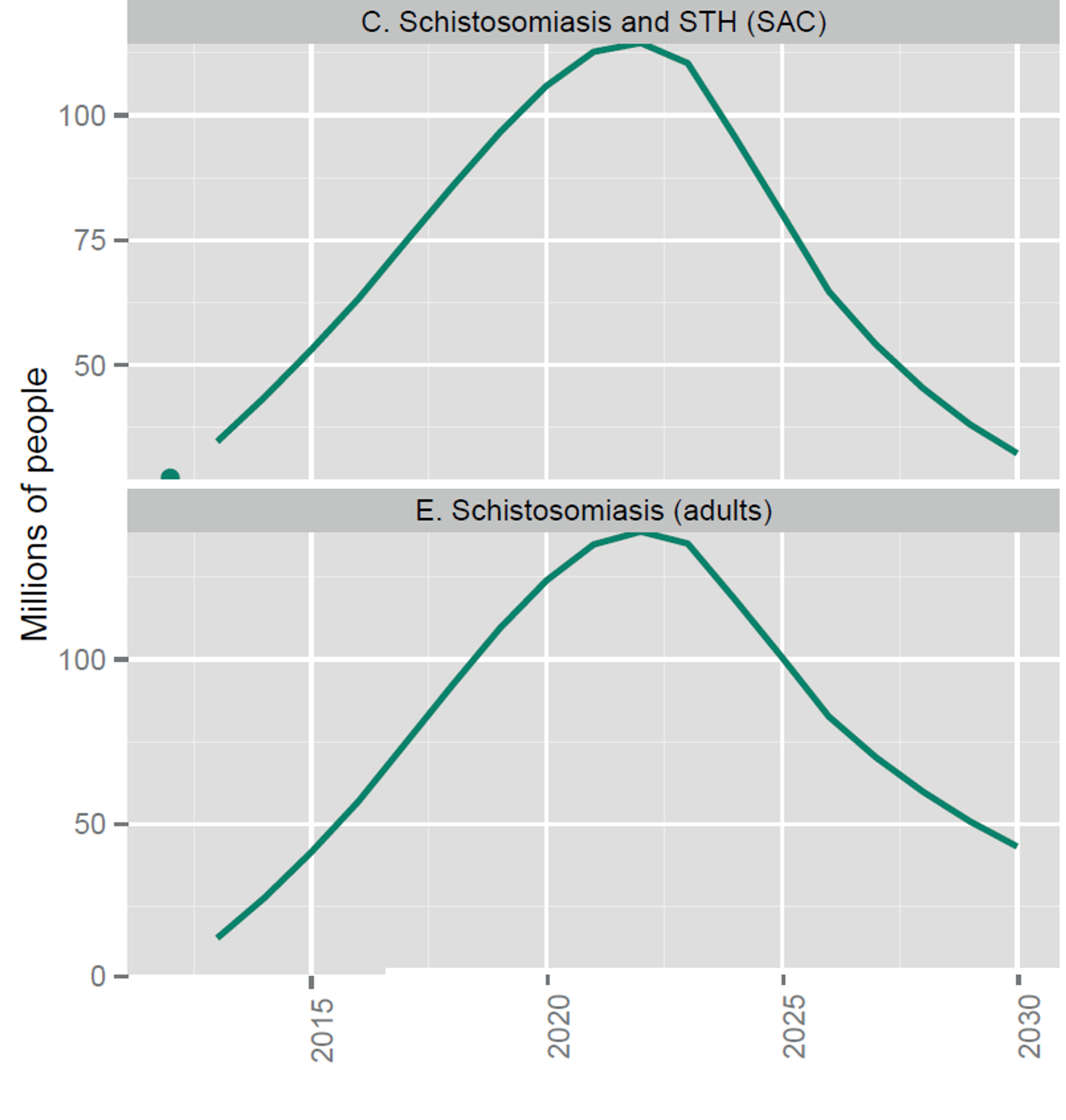
Fig. 1: Number of people targeted for coverage with integrated preventive chemotherapy, selected NTDs (from recent WHO report on NTDs [13])
Figure notes: school-age children; STH, soil-transmitted helminthiases.
Notes: The dots indicate the number of people treated in 2012; the solid lines are targets not forecasts. Targets assume integrated delivery of preventive chemotherapy for LF and onchocerciasis in Africa, schistosomiasis and STH among school-age children, and LF and STH outside Africa. Pending further evidence, they do not yet assume further integration of LF and onchocerciasis in Africa with schistosomiasis and STH.

Fig. 2: Figure showing the overall projected costs of all preventive chemotherapy (i.e. mass drug administration against NTDs including schistosomiasis and soil transmitted helminths) in the coming years. This excludes medicine prices, which are donated by the pharmaceutical companies. Figure adapted from (Fig. 2.4 Investment targets for universal coverage against NTDs from recent WHO report on NTDs [13]).
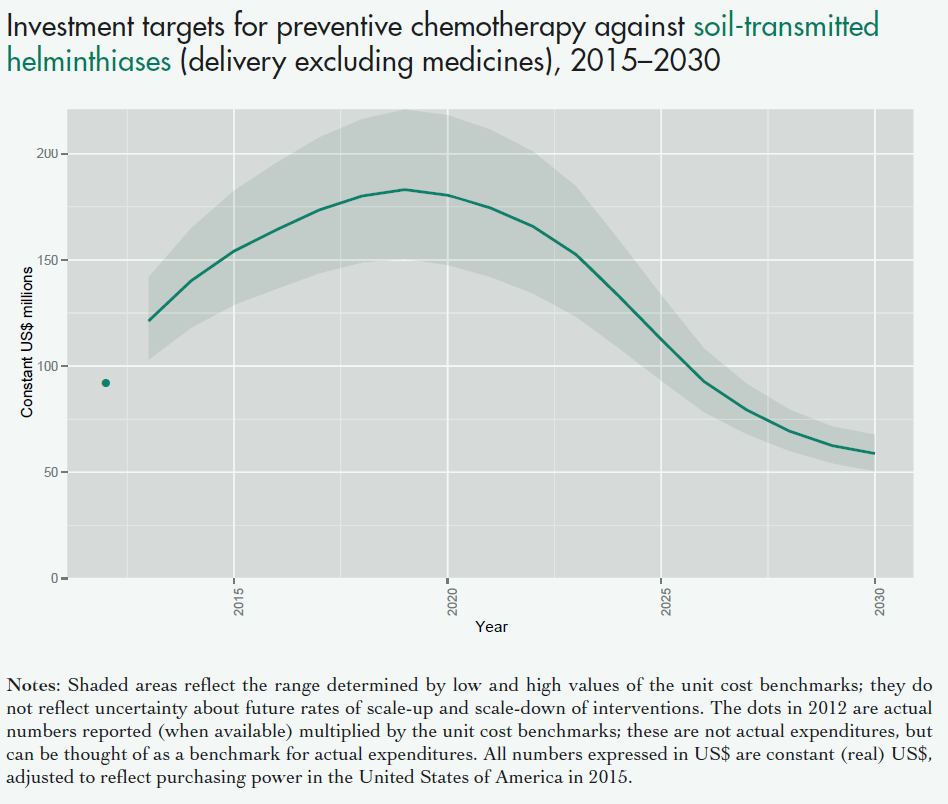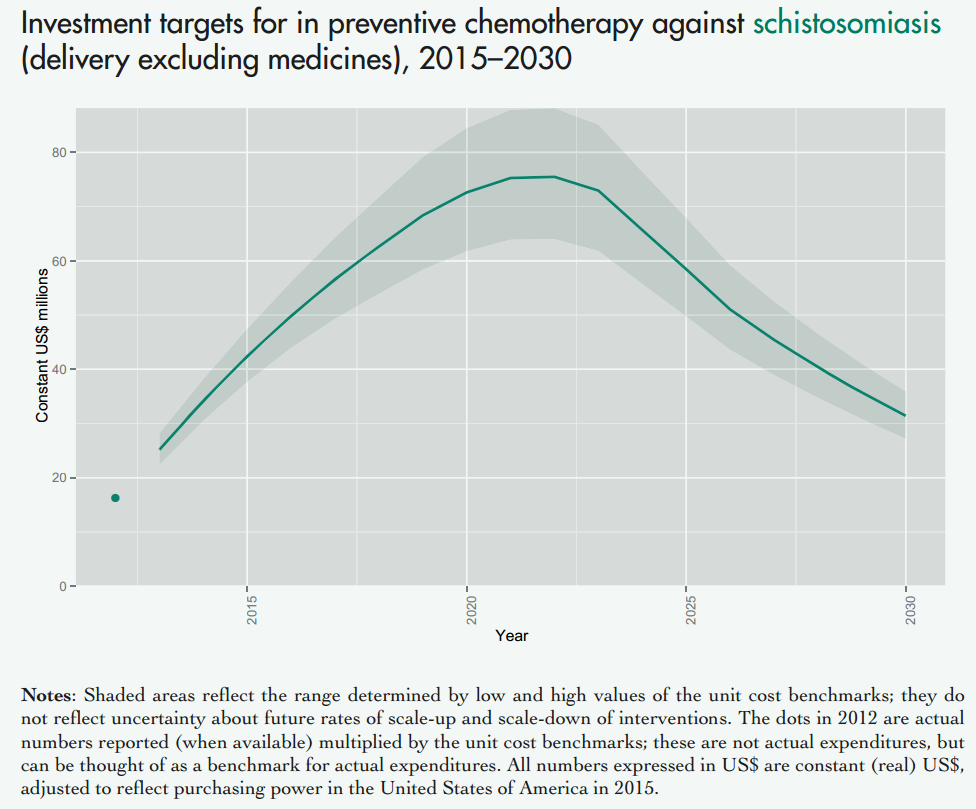
Fig. 3: Figure showing the projected costs of preventive chemotherapy against schistosomiasis (upper panel) and soil transmitted helminths (lower panel) in the coming years. This excludes medicine prices, which are donated by the pharmaceutical companies. Figure adapted from a recent WHO report on NTDs [13].
Notes: Shaded areas reflect the range determined by low and high values of the unit cost benchmarks; they do not reflect uncertainty about future rates of scale-up and scale-down of interventions. The dots in 2012 are actual numbers reported (when available) multiplied by the unit cost benchmarks, which is the approximate cost of delivering one treatment; these are not actual expenditures, but can be thought of as a benchmark for actual expenditures. All numbers expressed in US$ are constant (real) US$, adjusted to reflect purchasing power in the United States of America in 2015.
Updates on Fundraising Activities
SCI has been very successful at starting partnerships and receiving funding from governmental and non-governmental organisations. However, based on their effectiveness, reputation, and room for additional funding, one might have expected then to have received more funding from private foundations and private donors in recent years. Based on conversations with SCI, they are currently working closely with the Imperial College Development Office team on increasing their efforts to attract grants from private foundations and philanthropists. They are also in the process of hiring additional staff for their Fundraising and Advocacy team. At Giving what we can we assess charities on their effectiveness and not exclusively based on overhead costs, so we think using resources to attract more funding can potentially be a very good idea.
Updates on Expertise
Recently, SCI has hired more staff for their operations. The five new hires have graduate degrees and among them are a biostatistician, who has published in peer reviewed journals, and an expert on the link between schistosomiasis and HIV infections (an important topic on which we have previously reported). We believe that it reflects well on SCI that they continue to expand their team with the needed expertise.
Updates on SCI’s Plans and Activities from November 2014 to March 2015
In most of the 16 countries that SCI operates in, the deworming programs are going according to plan, according to SCI [14]. However, there were problems with deworming programs in three countries. In Liberia, due to the Ebola epidemic, all deworming operations have been suspended. In Yemen, due to political tension, a staff member had to be temporarily evacuated last year, but has now resumed work. In Zambia, drug delivery seems to be a continuing problem: SCI reported in April 2014 [15] that, due to delays during 2013, treatment scheduled across 6 provinces only took place between January - March 2014. The remaining 4 provinces were scheduled to receive MDA during July 2014. However, then in December 2014, SCI reported that only “piecemeal treatments” – about 60,000 – were successfully delivered.
Overall, we feel that, since there were only 3 out of 16 countries in which operations had problems, and some were due to reasons that were hard to predict, SCI’s operations seem to run very well.
The Upshot
In sum, SCI continues to be one of the most effective charities in the world. Its operations are very well executed and this is likely to continue as SCI has recently hired new, highly qualified staff. Recent scientific findings suggest that treating schistosomiasis might reduce - with great effectiveness - both malaria and HIV infections, which might make SCI even more effective than we previously thought. Finally, both in the short, but especially in the long-term, we believe that there is room for millions of dollars of additional funding and therefore we strongly recommend SCI as a charity to donate to.
References
- Mbah, Martial L Ndeffo et al. "Potential cost-effectiveness of schistosomiasis treatment for reducing HIV transmission in Africa–the case of Zimbabwean women." PLoS neglected tropical diseases 7.8 (2013): e2346.
- Mbah, Martial L Ndeffo et al. "Impact of Schistosoma mansoni on Malaria Transmission in Sub-Saharan Africa." PLoS neglected tropical diseases 8.10 (2014): e3234.
- Mbah, Martial L Ndeffo et al. "Cost-effectiveness of a community-based intervention for reducing the transmission of Schistosoma haematobium and HIV in Africa." Proceedings of the National Academy of Sciences 110.19 (2013): 7952-7957.
- Morrow, Richard H, Robert L Colebunders, and James Chin. "Interactions of HIV infection with endemic tropical diseases." AIDS 3.1 (1989): S79-88.
- Feldmeier, H, I Krantz, and G Poggensee. "Female genital schistosomiasis as a risk-factor for the transmission of HIV." International journal of STD & AIDS 5.5 (1994): 368-372.
- Li, Xin-Xu, and Xiao-Nong Zhou. "Co-infection of tuberculosis and parasitic diseases in humans: a systematic review." Parasit Vectors 6.1 (2013): 79.
- Gasim, Gasim I, Abdelhaleem Bella, and Ishag Adam. "Schistosomiasis, hepatitis B and hepatitis C co-infection." Virology Journal 12.1 (2015): 19.
- Botes, SN et al. "Schistosoma Prevalence in Appendicitis." World Journal of Surgery (2015): 1-4.
- McCreesh, Nicky, Grigory Nikulin, and Mark Booth. "Predicting the effects of climate change on Schistosoma mansoni transmission in eastern Africa." Parasites & vectors 8.1 (2015): 4.
- Neves, Bruno J, Carolina H Andrade, and Pedro VL Cravo. "Natural Products as Leads in Schistosome Drug Discovery." Molecules 20.2 (2015): 1872-1903.
- Kasinathan, Ravi S, William M Morgan, and Robert M Greenberg. "Genetic knockdown and pharmacological inhibition of parasite multidrug resistance transporters disrupts egg production in Schistosoma mansoni." PLoS neglected tropical diseases 5.12 (2011): e1425.
- Daumerie, Denis, and Lorenzo Savioli. Working to overcome the global impact of neglected tropical diseases: first WHO report on neglected tropical diseases. David William Thomasson Crompton & Patricia Peters. World Health Organization, 2010.
- World Health Organization. Investing to overcome the global impact of neglected tropical diseases 2015.
- SCI newsletter: December 2014
- SCI newsletter: April 2014